
Skull Density Ratio (SDR) and MR Guided Focused Ultrasound – What is it and why is it needed?
MR-Guided Focused Ultrasound (or MRgFUS) is a pioneering non-invasive form of neurosurgery for the symptoms associated with Essential Tremor and Tremor-Dominant Parkinson’s Disease.
MRgFUS is a fusion of two well-recognised technologies;
- Magnetic Resonance Imaging (MRI), which is used to create high resolution images to visualise a target in the deep brain brain called the Ventral Intermediate Nucleus, and
- Ultrasound, which is used to direct energy very precisely to that target, with the aim of destroying a small number of cells and interrupting the signals that are driving a patient’s tremor.
One of the key benefits of MRgFUS is that unlike other types of functional neurosurgery, focused ultrasound does not require any incisions or cuts in the scalp, or any holes made in the skull. This means that recovery is quick and there is no need for any general anaesthetic. However, this does mean that the success of MRgFUS is reliant on the ultrasound waves passing through the bone of the skull and reaching the intended treatment area with enough energy to produce the intended result. Since bone absorbs and deflects ultrasound waves, this presents quite a challenge for neurosurgeons and neurologists involved in MRgFUS treatment. However, a simple scan can help!
Assessing skull density using CT scanning
All patients who are being considered for focused ultrasound thalamotomy for Essential or Parkinsons Tremor will undergo a range of investigations as part of their pre-treatment assessment. This normally involves a combination of consultations with the treatment team and imaging tests, which will include an important CT scan of the skull.
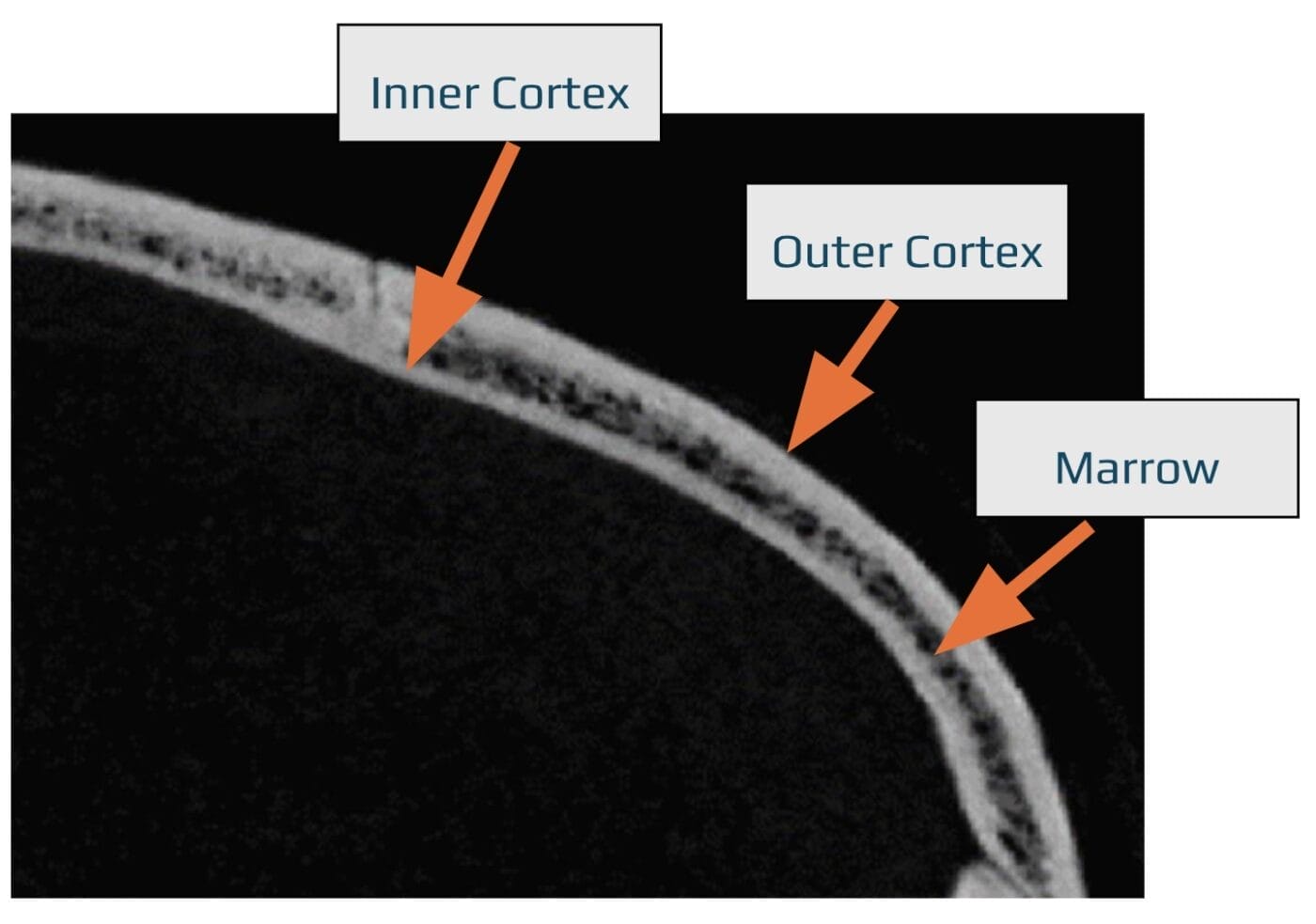
CT scans provide detailed images of the skull’s structure which is not necessarily the solid bone that you might expect. In fact, the multiple bone ‘plates’ that form the skull are each made of different types of bone. Dense cortical bone forms an outside protective layer, preventing bending and twisting and providing strength and protection to the bone and to the internal organ it is protecting. However, between the two layers of cortical bone sits softer, spongy bone marrow, which make the skull bones lighter, whilst also being involved in the formation of red and white blood cells.
The density and thickness of skull bone varies greatly from one part of the skull compared to another and will be different in one patient compared to another. Human skulls are each unique and are strongly influenced by age, gender and genetic factors, with skull size and shape varying depending on where in the World the patient is from.
To overcome this variability, a CT scan can be used to provide detailed images of the skull’s structure, allowing us to map the density and thickness of the bones in an individual patient and plan the exact power and trajectory of the ultrasound waves needed to deliver the perfect amount of energy directly to the target area.
The impact of Skull Density Ratio and its effect on treatment
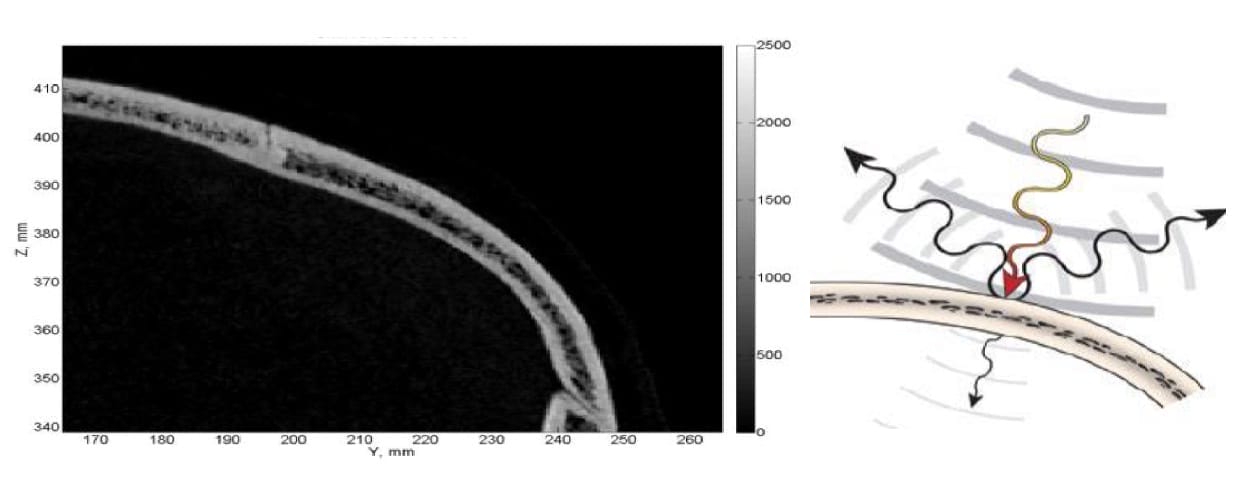
With the images created from the CT scan, a parameter known as Skull density Ratio (or SDR for short) can be calculated. Mean SDR quantifies skull density by looking at the proportion of marrow to cortex and helps predict how much ultrasound energy will be absorbed or deflected by the skull (influencing how effective treatment can be) in an individual patient.
In general, a lower SDR means that more ultrasound will be deflected and absorbed by the patient’s skull. This means that there is a higher risk of inadequate energy delivery to the target area, or unintentional heating or surrounding structures which could lead to adverse effects. Whist it may still be possible to tailor the treatment plan accordingly, a patient with a low SDR may possibly be considered technically less suitable for focused ultrasound treatment.
Low SDR
On the other hand, a higher SDR means that more of the ultrasound waves will be able to pass through the skull and reach the intended target. The surgeon will be more able to reach the intended target with the prescribed amount of energy, achieving the desired outcome with a lower risk of any adverse effects. This means that the patient is technically suitable for focused ultrasound treatment.
High SDR

Conclusion
CT scans play a vital role in the successful treatment of patients using MR-guided focused ultrasound. Whist the result of the CT scan is just one of several pieces of information which will be used by the treatment team to decide whether or not MRgFUS is a suitable treatment option for a specific patient, it can help with the selection of patients and the planning of treatments so that parameters and trajectories can be adjusted to minimise any possible risks. Mean SDR calculation from CT scanning is just one of several examples where MR guided focused ultrasound thalamotomy is tailored and personalised to each individual, maximising treatment outcomes and safety, whilst minimising the risk of potential adverse effects.
MORE NEWS

